Acute Osteotomy
Elizabeth W. Hubbard, MD
What is an osteotomy?
An osteotomy is when a surgeon cuts a bone into 2 or more segments. This is a careful intentional break in a bone. This is usually done when there is a problem with the shape or alignment of the bone. The bone either has an unusual angle or length that needs to be corrected or sometimes the bone can be abnormally rotated (Figure 1). Osteotomies allow a surgeon to manipulate and realign the bone. Realignment can be done acutely or gradually. An osteotomy with acute realignment means that the surgeon will cut the bone and at the same time correct (straighten a crooked bone) the angle or rotation of the bone immediately in the operating room. The bone is then held in its new corrected position with internal or external hardware such as plates and screws, an intramedullary nail or an external fixator (Figure 1). An osteotomy with gradual realignment means that that the surgeon will cut the bone at the time of surgery but that the actual correction of the shape of the bone will happen slowly over time, usually with the assistance of a special type of external fixator such as a circular external fixator (Figure 2).
Figure 1
12-year-old with left leg genu valgum (knock-knee deformity) due to a problem with the left femur (1a). Preoperative planning shows that the weight bearing axis of the right leg falls close to the center of the knee joint, but on the left side this line falls outside the knee joint (1b). Intra-operative x-ray after an acute osteotomy of the femur shows improved alignment (1c).
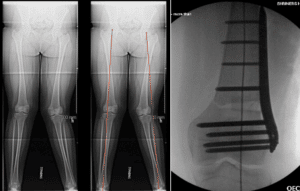
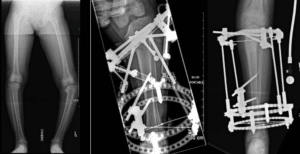
Figure 2 10-year-old with an angular deformity of the left tibia (2A). The deformity was felt to be too severe for an acute osteotomy so gradual correction using an external fixator was performed. Figures 2B and 2C demonstrate the alignment of the tibia at the time of frame application and at the completion of correction, respectively.
How does the surgeon decide whether the bone should be corrected acutely or gradually?
Usually mild problems with bone angulation or rotation can be corrected at the same time that the surgeon cuts the bone, which would be an acute osteotomy. Acute osteotomy of severerly crooked bones can result in significant swelling, and/or stretching of soft tissues such as skin, blood vessels and nerves. Patients who have severe deformities or leg length issues will often be treated with a gradual correction. In these situations, a gradual correction of the deformity done after the bone is cut can often be safer because it places less stretch on the bone, muscles, nerves and blood vessels during the correction process. It also allows for the formation of new bone when this is desired, such as a limb lengthening procedure.
Why would I or my child need this?
Common reasons to need an osteotomy include:
• You or your child has a bone that has an abnormal angular deformity, such as bow legging or knocked knees (Figure 1)
• You or your child has a rotational deformity of the femur or tibia that results in problematic in-toeing or out-toeing
• You or your child had an injury that resulted in an angular, length and/or rotational deformity that will not correct on its own. Leaving these deformities untreated could place you or your child at risk for functional and degenerative problems as time goes on (Figure 3)
Figure 3 12-year-old female broke her left ankle, injuring the tibial growth plate close to her ankle joint. Her fracture healed well in a cast (3A). However, x-rays 6 months later showed that she had developed a growth arrest in the anterior aspect (front) of her growth plate, changing the alignment of her ankle joint (3B). She was taken to the OR for an acute osteotomy to restore her alignment (3C). At the same time, a procedure was done to close the posterior growth plate of the tibia to prevent recurrence of the deformity (3C).

How is an osteotomy done?
A bone can be cut using different types of oscillating saws, a flat metal chisel like instrument known as an osteotome, or a chord like saw called a gigli saw. Your surgeon will often use intraoperative x-ray (fluoroscopy) to ensure both correct placement and completion of the osteotomy and appropriate correction of the deformity. An acute osteotomy means that the surgeon will need to somehow hold the 2 pieces of the bone in the new, corrected position so that they can heal appropriately. This usually involves placing either wires, plates and screws, an intramedullary nail, or an external fixator to stabilize the bone. Sometimes external fixators are placed on the limb during the procedure to hold the bone in place, and then removed after the plate and screws or intramedullary nail is placed. You or your child may also need to be placed in a splint or cast after surgery to help protect the surgery site so that it can heal. The location of the osteotomy and type of implant that is used to stabilize the bone usually determines if you or your child will need a splint, cast or brace after surgery and what type of splint, cast or brace you might need.
What are the general benefits of this procedure?
An acute osteotomy means that the angular or rotational problem in the bone is corrected during the surgery, so the deformity will be corrected when you or your child awakens from surgery. You or your child typically do not need further surgery for this problem unless (1) the implants used at the time of surgery need to be removed or (2) your or your child’s underlying condition is complex and requires multiple interventions. The need for further surgery is patient and condition dependent and your surgeon should discuss any potential need for further surgeries with you prior to the osteotomy.
What are the general risks of the procedure?
With an acute osteotomy, the underlying angular or rotational problem in the bone is fixed at the same time that the surgeon cuts the bone. This means that the surgeon is intentionally creating a fracture (or broken bone) and then immediately stabilizing it. Slow or incomplete bone healing can occur and may require more surgery. Just like with traumatic breaks in bones, this procedure can result in a lot of swelling. This swelling can increase the pressure at the site of the osteotomy, meaning that the muscle can swell and there can be pressure placed on arteries, veins, and nerves. When the swelling is significant, this is called a compartment syndrome. If a compartment syndrome is not recognized early, the swelling can actually cause significant damage to the muscles, arteries, veins and nerves at the site of the surgery and potentially result in significant permanent damage.
Even in the absence of significant swelling, correcting a large angular or rotational deformity can sometimes cause the surrounding blood vessels and nerves to be stretched. This can cause damage to the blood vessels and nerves. This could result in temporary or permanent numbness or loss of muscle strength or function. Correcting a large deformity can also stretch the skin, which might make it difficult for the skin to heal after surgery.
Because of the risks of injury with acute osteotomies, only relatively small angular or rotational problems in bones can be corrected acutely, meaning at the time of the osteotomy. Large angular or rotational deformities often need to be corrected gradually meaning that the bone is cut and then the angular and/or rotational deformity is corrected slowly, starting 5 to 10 days later, using either an external fixator or an intramedullary nail with moving parts (Figure 2). Gradually correcting an angular or rotational deformity places less stretch on the muscles, blood vessels and nerves and is often safer for larger deformities.
The decision of whether to do an osteotomy acutely or gradually depends on the location of the deformity and the severity of the deformity. Your surgeon will discuss the options with you prior to surgery so that the correct procedure is performed.