Congenital Posteromedial Bowing of the Tibia
Reid Nichols, M.D.
Introduction
Congenital posteromedial bowing of the tibia (CPMBT) is a relatively uncommon congenital anomaly which usually affects one leg. The foot and bones of the lower leg are deformed. The foot is often touching the front of the shin bone and appears similar to a condition called calcaneovalgus foot, although in CPMBT the tibia bone is deformed while in calcaneovalgus foot the tibia bone is straight.


Anatomy
This deformity affects the two bones of the lower leg and the foot, the tibia and fibula. The shin bones have a characteristic bowing or bending inward towards the other leg (medial) when looking from the front of the body and backwards (posterior) from the side view.
Description
Posteromedial bowing of the tibia can be detected on an ultrasound prenatally. The left leg is affected more often than the right. The deformity of the foot and tibia will both improve with time, as shown in the x-rays below. The ankle range of motion may not be as flexible as the other leg. The foot and calf may be smaller as the child grows. Shortening of the tibia and fibula also typically occurs, generally ranging from 3 to 7 cm at skeletal maturity.
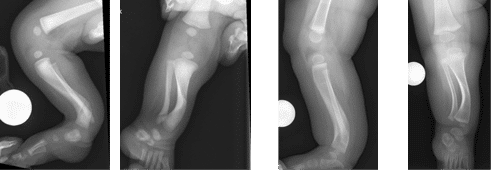
Figure 1: Age 2 weeks Figure 2: Age 8 months
Cause
The cause is not fully understood. A transient constriction by an amniotic band or other compressive event in utero may cause CPMBT.
Symptoms
No other conditions are associated with the CPMBT. The soft tissues in front of the ankle are tight and will need to be stretched. The overall length of the shin bone is shorter which can cause issues when the child begins to walk.
Doctor’s Examination
In addition to general exam, the doctor will perform a focused evaluation of the affected leg. The doctor will check range of motion of the hip, knee, and ankle. It is common to have an X-ray to document the bowing of the leg.
Nonsurgical Treatment
CPMBT does not require immediate surgical intervention. Gentle stretching of the foot and ankle will improve the appearance of the foot. Some doctors may consider a cast or splint to help stretch the foot and ankle. When the child is walking, a shoe lift may be used to compensate for limb length inequality.
Surgical Treatment
There is often a residual bend in the tibia and fibula and restricted range of motion of the ankle. The leg length discrepancy and residual angular deformity of the affected leg can be addressed with an osteotomy (bone cut) and lengthening. An external fixator may be used in this procedure to correct both simultaneously. The other leg can also be shortened to compensate for the length difference. This procedure is called an epiphysiodesis. It is a much more minor procedure, with the downsides that it does not correct any deformity of the bone and it results in less overall height.