Key Techniques: Bone lengthening with an Internal Lengthening Nail
Claire Shannon, M.D.
Paley Orthopedeic and Spine Institute
The basic principle of bone lengthening uses a biologic process called distraction osteogenesis. This can be performed when a surgeon cuts the bone with an operation in a specific way, called a corticotomy. The bone is allowed to heal for few days (latent phase), and then the immature healing bone is slowly pulled apart (distraction phase ). As the bone distracts, it forms a soft bone in the space created by pulling the bones apart (regenerate). This new bone eventually heals and hardens (consolidation phase). This has traditionally been a procedure that has required external fixators with moving parts. New technology permits some bone lengthenings to be achieved without the external fixator. The advantages of internal lengthening compared to external fixators is the elimination of any external pins, wires or rings, and their associated risk of infections, unsightly scars and refractures after external fiaxtor removal.
There have been a number of internal devices developed since the introduction of internal limb lengthening. The original models made use of a ratcheting device that required rotation of the nail, and therefore the leg, to perform the bone lengthening. Newer technology uses rotating spindles, activated by either an electric current or by magnetic field from an external remote control (ERC). The goal of all of these devices is to perform gentle, controlled distraction of the bone to lengthen the limb and avoid the risks of infection and soft tissues tethering from pins incurred with external fixation. The following technique will assume use of a magnetic internal lengthening nail.
The femur (thigh bone) is the most commonly lengthened bone with internal nails. This can also be done to the tibia (shin bone) and the humerus (upper arm bone) (Fig 1).
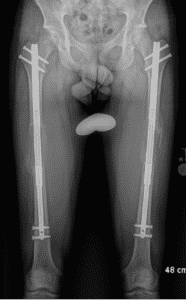

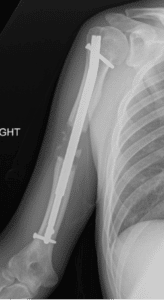
Fig 1: Left – Bilateral femoral lengthening nails. Center – Right tibial lengthening nail. Right – Right humeral lengthening nail
Patient Selection
In general, lengthening surgery is done for limb length inequalities greater than 2 cm. This may be due to many different causes, such as congenital (starting from birth) limb differences, trauma, illness, infection, or genetic disorders. The basic criteria to perform internal lengthening is the ability to place the device inside the canal of the bone. Therefore, the bone to be lengthened must be large enough in length and diameter to accept the implant, as well as not having growth plates that can be injured during insertion. An additional consideration is the size of the soft tissue envelope, as the external device that directs the lengthening process must be able to activate the nail in order to effect lengthening.
In some cases where the bone shape or diameter cannot accommodate a nail inside the bone, or where an active growth plate is blocking entry to the bone, a special technique called Extramedullary Internal Lengthening (EMIL) can be used. The lengthening nail is attached to the outside of the bone, but under the skin and muscle (Fig 2). A small metal rod is often inserted inside the bone to help keep the bone straight as it lengthens. The bone is cut and lengthened. In the same way as the intramedullary nail. A major limitation of this technique is that the patient cannot put any weight on their leg during the lengthening due to decreased stability of the nail compared to when it is inside the bone. Although this is a newer technique, the early results have been promising.
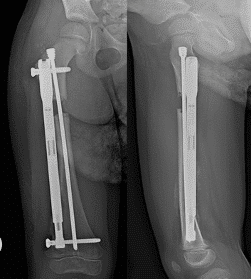
Fig 2: AP and lateral radiographs demonstrating placement of the lengthening nail for EMIL technique
Lengthening is a major reconstructive procedure and requires significant time and effort on the part of the patient to ensure successful outcomes. This means participating in physical therapy daily, including stretching and exercises at home. The lengthening of the bone is done at home by the patient (or parent), and must be done as prescribed. Patients, and their families in the case of pediatric patients, should demonstrate a clear understanding of the process, including the follow up schedule, the physical therapy requirements, and use of the ERC.
Surgical Procedure
The procedure may be combined with correction of a deformity if present. The surgery will take a few hours and will be performed in a hospital. Most patients stay overnight for pain control and physical therapy.
In order to have a successful lengthening, the surgeon must address any tight soft tissues in the limb before inserting the nail. The most common releases are:
- Femur:
- Iliotibial (IT) band: tight band along the lateral thigh that connects between the hip and the knee. This is the most common release done.
- Rectus Femoris : a muscle that flexes the hip
- Hip Abductors: muscles that move the leg away from the midline of the body
- Tibia:
- Peroneal nerve : a nerve that controls foot movement and sensation that wraps around the fibular neck (the small bone on the outside of the knee)
- Gastrocnemius: the calf muscle, makes up part of the achilles tendon
The bone is cut and the nail is then inserted into the bone. If the bone needs to be realigned, this will be done at the same time. The nail is inserted though small incisions and held in place with screws near the top and bottom of the nail(Fig 3).


Fig 3: AP and lateral radiographs of an antegrade femoral lengthening nail taken on the day of insertion. Note the osteotomy in the upper third of the femur
Lengthening:
Lengthening of the limb starts about 1 week after the surgery. You will be given a remote device (ERC) that you will need to place over a spot on the limb marked by the surgeon (figure 2). This is where the motor is in the nail. The ERC will be programmed to lengthen the nail a small amount at a time, and you will do this multiple times a day as instructed. The lengthening generally is not very painful, but will stretch the muscles, and this becomes more noticeable later in the lengthening. It is very important that you do your prescribed exercises from physical therapy to avoid the muscles getting too tight. Your surgeon will see you frequently to check xrays to ensure that the nail is lengthening as prescribed, and to make sure that your bone is healing properly. Depending on the device being used, you may have to limit your weightbearing and use crutches or a walker.
The length of time it takes to lengthen a bone depends on how much length you want to achieve and the rate of lengthening. It is possible to lengthen a femur up to 1mm per day, while a tibia is generally lengthened more slowly. For complete healing, the general rule of thumb is that every 1mm takes 3 days total treatment time. For example, if you were going to lengthen a femur 30mm (or 3 cm): 30mm = 90 days to achieve length and heal the bone.
Complications:
Your doctor will explain the risks and complications of limb lengthening to you in detail. Some of the more common complications may include:
• Bleeding: Most patients do not require transfusions. This risk is higher when more than one bone is lengthened at the same time or if other procedures are done at the same time.
• Joint contracture: tight muscles and tendons around the hip, knee or ankle due to stretching of the soft tissues. This is prevented with physical therapy and preventive soft tissue releases
• Blood clot: this risk is lowered with the use of medications and early mobility.
• Nerve injury: this can happen at the time of surgery or during lengthening due to stretching. This is prevented by slow lengthening and preventive releases. During the lengthening process, if you develop new pain, numbness or tingling in the surgical limb, tell your surgeon right away.
• Bone healing problems: the bone may heal too slow or too fast. This may be due to many different factors and can be minimized by close follow up with your surgeon as instructed.
• Secondary deformities due to lengthening may happen as the bone gets longer. Your surgeon will monitor this, and sometimes additional corrective surgery is necessary after the length is achieved. In some cases this additional surgery is expected and discussed in advance.
Long term Outcomes:
Most patients are satisfied after undergoing limb lengthening. They can expect their limb to work more like normal, providing improved walking and running and less need for assistive devices such as shoe lifts or prosthetic limbs (Fig 4). Some patients may need multiple procedures throughout their lifetime if their limb length difference is very large or due to a congenital limb difference. These should be spaced out as much as possible to minimize the number of surgeries needed.



Fig 4: 9year old girl with congenital femoral deficiency who underwent lengthening of her lerf femur to equalize her leg lengths. Left – Preoperative standing radiograph demonstrates a 5.5cm leg length difference. Center – Standing radiograph of the same patient after completing a 6cm lengthening of the left femur to equalize her leg length at the end of growth. She had hemiepiphysiodesis of the left distal medial femur for mild genu valgum. Right – Standing radiograph of the same patient after consolidation of the femur and correction of her genu valgum. The lengthening nail and hemiepiphysiodesis plate were removed the next day.